Updated: 27 Dec. 2014
AND THE BEAT GOES ONThis new blog is to relate what I discovered
- When generous friends wrote Alberta's then Health Minister, Fred Horne asking for Esbriet to be funded for idiopathic pulmonary fibrosis (IPF), including Minister Horne's response when I contacted him directly.
- Interesting tidbits from additional medical research on IPF.
- How physicians vary in their approach to patients with IPF.
BACKGROUND
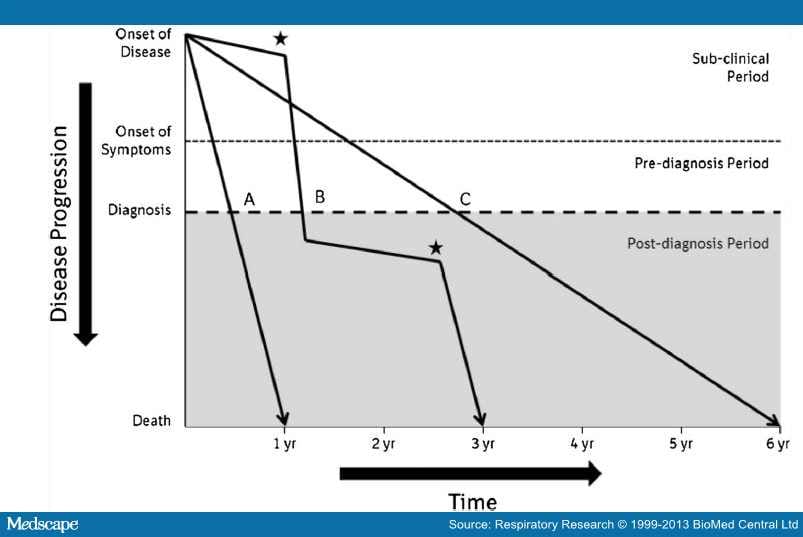
In 2013 my spouse was diagnosed with IPF, a deadly disease with no known cure and a median life expectancy after diagnosis of ~3 years.
Besides the diagnosis, it was a shock to learn that the one known treatment at the time (pirfenidone / Esbriet) was approved for use by Health Canada, but not funded by provincial governments.
I subsequently read many scientific papers on the issue and wrote 4 blogs that examined what it's like to get an IPF diagnosis and why Esbriet is covered by public funding in the UK but not Canada. In brief, reasons include
- The Canadian Drug Expert Committee (CDEC), under the auspices of CADTH, decided that Canada should not fund Esbriet (18 April, 2013).
- The clinical trial results at the time were equivocal and CDEC opted for seeing the glass half empty, no doubt partly because Esbriet is expensive ($40,000 - $50,000/yr). Provinces would prefer not to pay for a drug that slows, but does not cure IPF, a disease affecting mainly the elderly.
- To access the 4 earlier blogs on IPF: 'While my guitar gently weeps' (Musings on idiopathic pulmonary fibrosis).
Although we are fortunate to have great health insurance, it did not cover a drug as expensive as Esbriet. We understand why our drug maximum is $2000/yr, otherwise the plan would be unsustainable.
HOW GOVERNMENT RESPONDS
Many friends kindly wrote the Alberta government, usually the Health Minister, Premier, or their MLA, using a variation of the Canadian Pulmonary Fibrosis Foundations' provincial advocacy packages. Regardless of how personalized they made their appeals - including that they knew the UK but not Canada funded Esbriet - in return all, including me, received what amounted to a government form letter, which totally ignored the content of our letters.
In return I wrote Minister Horne and asked him to cut the crap and reply to 3 simple questions.
To his credit, Fred Horne replied to my direct questions. If I interpret Minister Horne's reply correctly:
- Unless CDEC recommends Esbriet funding, Alberta won't fund it.
- Alberta's expert committee (ECDET) accepts (rubber stamps) CDEC's decisions.
- Forget about Alberta's Short Term Exceptional Drug Therapy (STEDT), unless a drug is approved for public funding by CDEC OR Canada's provinces negotiate what they deem a reasonable cost for Esbriet.
Alberta Health's replies were as expected. I just wish the government would be more transparent and upfront, instead of giving citizens the hope that maybe you can get your expensive drug, with unknown or iffy efficacy, under special funding.
Maybe you can, but only if you are a cute child with a rare disease or if your disease is more common (e,g., cancer), thereby involving more voters. Cynicism or reality? You judge.
WHAT RESEARCH SAYS
Since I wrote the prior blogs, new research has emerged on Esbriet's value in treating IPF, notably,
- IPF now a treatable disease (CMAJ)
- Two drugs reduce the progression of IPF
- In 2014 The Journal of the American Medical Association (JAMA) reported that pirfenidone (Esbriet) reduced the relative risk of death or disease progression by 43% compared with placebo.
Accordingly, CADTH is looking at another submission on pirfenidone (Esbriet) and seeks input.
In the meantime, Esbriet's maker, Intermune was bought by Big Pharma's Roche for $8.3 billion, likely in the hope that the U.S. FDA will approve Esbriet for use in the USA. Effects of the takeover on Esbriet's public funding in Canada remain to be seen.
A TALE OF TWO PHYSICIANS
My spouse's initial lung specialist (pulmonologist / respirologist) is a physician with much experience, who gave Peter hope that he could get funding for Esbriet, which might significantly help, although not cure, his IPF. The doc patiently spent much time explaining IPF and its possible clinical courses.
He put us in touch with Esbriet's maker to investigate if our insurance would pay. He submitted Peter's name to Alberta's Short Term Exceptional Drug Therapy program (STEDT).
But he soon moved his practice outside our city to what is often called a 'bedroom community'. Although relatively close, driving is a challenge and I could not see travelling there for continuing care.
He put us in touch with Esbriet's maker to investigate if our insurance would pay. He submitted Peter's name to Alberta's Short Term Exceptional Drug Therapy program (STEDT).
But he soon moved his practice outside our city to what is often called a 'bedroom community'. Although relatively close, driving is a challenge and I could not see travelling there for continuing care.
Unfortunately, we quickly learned that Esbriet funding was a no-go (as explained above in correspondence with Fred Horne). The original respirologist was hopeful that it would eventually be funded, especially if enough people drew the Minister's attention to the issue of IPF and Esbriet / pirfenidone. Thus, we asked friends to write the Health Minister.
In a pulmonary care exercise program with an Edmonton primary care network, we were told that IPF could deteriorate quickly at any time (acute exacerbation), and we needed a physician to manage it. We opted for a respirologist who was younger and therefore the wait time to see her was less and was affiliated with the University of Alberta Hospital, the facility closest to us.
Her approach was caring but more or less 'all business' and straight forward.
We appreciated this approach: Let's assess the current state of the disease. What can we do, if anything?- She reassured Peter not to worry about no Esbriet funding. The drug is not a cure for IPF and has significant side effects.
- Her approach was, Let's take a few key tests (lung function, echocardiogram, CT scan, 6 minute walking test, review earlier sleep apnea test results) so that she could assess his current medical condition.
- Then she would discuss where he was at and treatment options.
LEARNING POINTS
Some of the key things we've learned:
1. Public advocacy programs for government funding of expensive drugs to treat incurable diseases are worthwhile but work better under certain circumstances.
- Many voters are mobilized to advocate the cause.
- Helps, but does not guarantee success, if
- Celebrities participate
- Disease is common
- Victims pull at heart strings
- Health Canada approval does not equal provincial funding.
- Governments seem content to let advocates 'piss in the wind' and only fess up to reality when pressed.
- Provincial exceptional drug therapy programs to fund high cost drugs for rare conditions do not apply to drugs unapproved for funding by CADTH's CDEC. [Except perhaps for children with heart-wrenching diseases like this little girl.]
- One approach does not fit all because communication involves a communicator (Dr.) and a recipient (patient), and recipients vary greatly in their ability to accept harsh facts.
- In our case a reality-based approach is okay.
- Canada's CDEC clearly puts cost-effectiveness first. No doubt cash-strapped provinces prefer this.
- Otherwise, why would the UK's NICE committee recommend funding Esbriet to treat IPF, and Canada's CDEC recommend the opposite, based on the same evidence?
- For the record, NICE's 64-page report is transparent and discusses all issues in detail. CDEC's report is 5 pages.
- UK experts noted that it was unlikely that clinical trials for IPF treatments can ever have enough statistical power to detect a difference in mortality. They recognized this limitation.
- Yet new studies show Esbriet reduced the relative risk of death or disease progression by 43% compared with placebo.
- Canada's experts chose to ignore statistical power.
- Statistical power: Ability of a study to detect a real difference, if one exists. Power is affected by how big the difference is and sample size. If a difference is big, it's easier to detect. And large sample sizes make a real difference easier to detect.
- In discussing why spouse's lung biopsy showed evidence of pulmonary hemorrhage, not one specialist could explain it.
- Seems medicine remains both a science and an art.
Miracle of miracles, early in Dec. 2014 we learned that the Alberta government would fund Esbriet under the STEDT program. For this we thank Peter's initial respirologist, Dr. Lyle Melenka. See
FOR FUN
As Peter and I deal with a diagnosis of an incurable disease, idiopathic pulmonary fibrosis, we focus on the glass half full. Every day, every month, every year is a blessing.
Which brings me to an old but fabulous Beach Boys ditty.
- Good vibrations (Love this song)
- Autopsies in acute exacerbation of idiopathic pulmonary fibrosis (Interesting findings. Perhaps they can be of use in treating IPF.)
- Acute exacerbation in idiopathic pulmonary fibrosis.
- Clear diagram of the 3 types of disease progression in IPF.
- Drugs for rare diseases. Evolving trends in regulatory and health technology assessment perspectives (CADTH, Aug. 2013)
- Quote in Summary on Alberta: 'A Short Term Exceptional Drug Therapy program for funding high-cost non-formulary drugs for rare conditions is available for both in-patients and outpatients.' [In theory, not in practice.]

{kind=link}
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.